INTRATUNNEL
PHACOFRACTURE: A NEW NUCLEUS MANAGEMENT TECHNIQUE OF MSICS
Intra tunnel phaco
fracture is a new technique nucleus management technique of the manual small
incision cataract surgery (MSICS). Other commonly practiced MSICS techniques
are Blumenthal, visco-expression, irrigating wire vectis and fish hook needle.
These techniques require a 7 to 9 mm large incision, which leads to more
astigmatism. Intratunnel phaco fracture is a new technique innovated by Dr
Sudhir Singh, where the lens nucleus is broken inside the sub 6 mm
sclerocorneal tunnel. All types cataracts nucleus can be taken out easily
through 4.5 mm to 6.00 mm wide corneoscleral tunnel. We are going to
demonstrate this technique in this article
Keywords: MSICS,
intratunnel, phacofracture,
Introduction
The
cataract remains the leading cause of avoidable blindness in the world. According to the latest assessment, cataract is
responsible for 51% of world blindness, which represents about 20 million
people (2010). Although cataracts can be surgically removed, in many countries
barriers exist that prevent patients to access surgery. Manual small
incision cataract surgery (MSICS)
and phacoemulsification are the most popular methods of cataract extraction
today. MSICS is significantly
faster, less expensive and less technology-dependent than phacoemulsification.
MSICS has been extensively practiced in developing countries like India. Intratunnel phaco fracture is a new
nucleus management technique, where the lens nucleus is broken inside the sub 6
mm sclerocorneal tunnel and removed in contrast to other contemporary
techniques. This is our original technique.
Intratunnel Phacofracture Technique
Intratunnel phaco fracture
nucleus management technique was first described by author1.Its a
simple, inexpensive reproducible technique. Per case consumable expenditure of
cataract extraction using this technique is given in table 1.
S.N
|
Consumables Name
|
Consumables Cost In USD
(in India)
|
Consumables Quantity
|
Total Cost In USD (in India)
|
1.
|
15 degree blade
|
0.5
|
1
|
0.5
|
2.
|
Crescent Blade
|
0.5
|
1
|
0.5
|
3.
|
2.8 mm Keratome
|
0.5
|
1
|
0.5
|
4.
|
5.0 mm Keratome
|
0.5
|
1
|
0.5
|
Drip Set
|
0.5
|
1
|
0.5
|
|
5.
|
Viscoelsatics (HPMC )
|
1.0
|
1
|
1.0
|
6
|
Ringer Lactate Solution
|
0.5
|
1
|
1.0
|
Trepan Blue
|
0.5
|
1
|
1.0
|
|
IOL
|
3.0
|
1
|
2.5
|
|
Medication
|
2.5
|
2.0
|
||
Total
|
10.0
|
First postoperative day
visual outcome of 6 mm intratunnel phacofracture is given in table 2 and 3.
Table 2. First postoperative day uncorrected visual acuity(UCVA)
following 6 mm intratunnel phacofracture technique
|
||
Visual Acuity
|
Patient Number (%)
|
Patient Cumulative
Number (%)
|
6/6
|
7(5.14)
|
7(5.14)
|
6/9
|
29(21.32)
|
36(26.47)
|
6/12
|
32(23.52)
|
68(50.00)
|
6/18
|
48(35.29)
|
116(85.29)
|
6/24
|
16(11.76)
|
132(97.05)
|
6/36
|
4(2.94)
|
136(100)
|
(Source: US Ophthalmic Review, 2014; 7(1):26–30)
Table 3. First postoperative day best corrected
visual acuity(BCVA) following 6 mm intratunnel phacofracture technique
|
||
Visual Acuity
|
Patient Number (%)
|
Patient Cumulative
Number (%)
|
6/6
|
20(14.70)
|
20(17.17)
|
6/9
|
56(41.17)
|
76(55.88)
|
6/12
|
48(35.29)
|
124(91.17)
|
6/18
|
9(6.61)
|
133(97.79)
|
6/24
|
1(0.73)
|
134(98.52)
|
6/36
|
2(1.47)
|
136(100)
|
(Source: US Ophthalmic Review, 2014; 7(1):26–30)
The mean uncorrected visual acuity and
mean best corrected visual acuity at first post operative day were 0.367 (Snellen equivalent 20/46) and
0.226(Snellen equivalent
20/33) log MAR units respectively. No serious per and
post operative complication encountered1.
Anesthesia
Manual small incision can be done performed under
peribulbar or topical anesthesia.
Site
of Incision
Site of incision is chosen
according keratometry values (K1and K2).The superotemporal quadrant for right
eye and the superonasal quadrant for left eye should be chosen if K1 and K2
difference is equal or less than 1.0 diopter (Figure 1).

Figure 1
If K1 and K2
difference is more than 1.0 diopter then incision should be on steeper axis
made. If K1 is steeper than K2 then superior incision (Figure 2) and If K2 is
steeper than K1 then temporal incision (Figure 3).

Figure 2

Figure 3
Ads by google
Ads by google
Ads by google
Surgical Steps
Cleaning and draping
The skin of the eyelids, lid margins and around the
eye is cleaned with 10 percent solution of povidone-iodine
solution. Drape is applied. Wire speculum is placed. Cul de sac is thoroughly
washed with Ringer’s lactate solution or balanced salt solution.
Superior
Rectus Bridle Suture
A 4/0 silk superior rectus bridle suture is placed
beneath the tendon of the superior rectus muscle. It is helpful to positioning
eye after local anesthesia. Superior rectus bridle suture is not used when
surgery is planned under topical anesthesia.
Conjunctival
Flap
A fornix based conjunctival flap at the limbus with a
chord length of approximately 6.5 mm was made. After careful dissection of the
Tenon’s capsule, light cautary was applied (Image 4).

Image 4
Sclera-corneal
Tunnel
A 6 mm scleral frown incision, 1.5 mm from the limbus is made
with a 15 number Bard Parker blade (Image 5). A funnel shaped sclerocorneal tunnel
incision is created with a steel crescent knife. One side port is made 90
degrees apart on either side of the scleral tunnel with a 15 degree knife
temporally in right eye and nasally in left eye. With a 2.8 mm keratome, the
anterior chamber was entered 1.5 mm into the clear cornea. Anterior chamber is entered with 1.5 mm in clear
cornea with help of 3.2 mm keratome (Figure 6).
The hydroxyl propyl methyl cellulose 2 % (HPMC) viscoelsatics is injected into
anterior
chamber.

Image 5

Image 6
Central Circular Capsulorhexis
The central circular capsulorhexis
is made with help of 26 gauze needle capsulotome. If glow is poor then capsule
was stained with trypan blue dye under the air bubble. Then viscoelsatics is
injected and capsulorhexis is made. The size of capsulorhexis is depends on the
size of the nucleus .It may vary from 5.5 mm to 7.5 mm (Figure 7). If nucleus
size was anticipated large then two relaxing incisions are made at the margins
of the capsulorhexis. Capsulorhexis can also be made by capsulorhexis forceps.

Image 8
Hydrodissection Procedure
The Hydrodissection is made
with 26 gauze cannula place on 2 CC syringe filled irrigating fluid.
Nucleus Prolapse in the Anterior Chamber
The internal incision of the tunnel was enlarged sideways to
7 mm the 5.1 mm keratome (Image 8) .Anterior
chamber is formed again with viscoelsatics and the nucleus is rotated within
the capsule using a Sinskey hook. The nucleus was prolapsed into anterior
chamber using a Sinsky hook. A Sinskey hook was used to retract the capsulorhexis
to engage the equator and lever out one pole of the nucleus outside the
capsular bag and the rest of the nucleus was rotated into the anterior chamber.
If the nucleus was too large then two or
three relaxing incision were made at the capsulorhexis margins at
equidistance (Image 9).

Image 8

Image 9
Google ads
Google ads
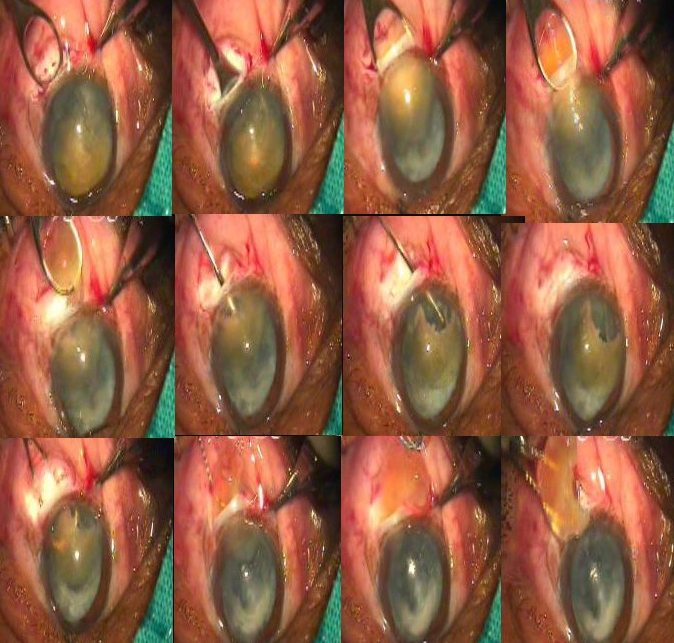
Nucleus Management
Up to this step all above
mentioned steps are same as in other manual small incision techniques. Intratunnel phacofracture technique is different than other
phacofracture techniques of anterior chamber. Enough viscoelsatics is placed
between cornea and superior surface of the nucleus to protect endothelium;
between nucleus and iris to keep away iris from nucleus. The nucleus is rotated within the capsule using a Sinskey hook.
The globe was stabilized with tooth forceps and the small Lewis lens loop (AA
1915 from Appasamy Associate, India) is introduced through the tunnel and positioned between
the iris and the nucleus. The nucleus is engaged in the lens loop and slowly
withdrawn from the anterior chamber while the posterior lip of the tunnel is
depressed. Once the nucleus got engaged in the tunnel, then the Lewis loop is pulled
posteriorly and upwards. This causes breaking and removal of a part of the
nucleus and other part remains engaged in the tunnel. By viscoelsatics the
engaged part of the nucleus is pushed back into the anterior chamber and
rotated so its longitudinal axis was coincided with longitudinal axis of the
tunnel. Again viscoelsatics is placed between the cornea and superior surface
of the nucleus and between the nucleus and iris. The lens loop is introduced
through the tunnel and positioned between the iris and the remaining part of
the nucleus. The remaining part of the nucleus is engaged in the lens loop and
slowly withdrawn from the anterior chamber while the posterior lip of the
tunnel was depressed. Most of the times remaining part of the nucleus comes
out. If it still break down then remaining part again pushed in the anterior chamber
with help of viscoelsatics and previous steps were repeated till it comes out (Figure
10).
Cortical Matter Clean Up
The remaining cortical matter clean up is
done with direct 23 gauge Simcoe irrigating aspirating cannula. The anterior chamber is formed with Viscoelsatics (Image 11).

Image 11
Intraocular
Lens Implantation
A single piece PMMA
intraocular lens of 5.5-6.00 mm optic size and 12.5 mm total size is implanted
into the capsular bag. The anterior chamber is washed
out thoroughly by Simcoe irrigation aspiration cannula using Ringer’s lactate
solution (Image 11).
Conjunctival
Flap Reposition
The conjunctival flap is reposited back and cauterized at the
edges.
Main
Ports and Side ports Sealing
Main port and side ports are sealed with stromal hydration
using a 26 gauze cannula.
Subconjuctival Injection
A 0.5 cc
subconjuctival gentamycin with dexamethasone injection is given. Eye is pad
patched
Discussion
The most
commonly practiced MSICS techniques are Blumenthal, visco-expression,
irrigating wire vectis and fish hook needle. These techniques require a 7 to 9
mm large incision, which leads to more astigmatism. So if nucleus is managed to
remove though a sub 6mm incision at appropriate site would result approximately
same astigmatism as 3.2 mm phacoemulsification 2-5. Intratunnel phaco fracture is a new
technique innovated by Sudhir Singh, where the lens nucleus is broken inside
the sub 6 mm sclerocorneal tunnel and removed. As nucleotomy maneuvering taken
place inside the corneo-scleral in contrast to other nucleotomy techniques
where maneuverings take place inside the anterior chamber. By
Intratunnel phacofracture technique all types of the cataracts were
successfully taken out through sub 6 mm wide tunnel. The mean
uncorrected visual acuity and mean best corrected visual acuity at first post
operative day were 0.367 (Snellen
equivalent 20/46) and 0.226(Snellen
equivalent 20/33) log MAR units respectively.
No serious per and post operative complication encountered.
FINANCIAL DISCLOSURE
The author has no
financial interest in any product mentioned.
References
- Sudhir Singh.
First Postoperative Day Visual Outcome Following 6 mm Manual Small
Incision Cataract Surgery Using Intratunnel Phacofracture Technique. US
Ophthalmic Review, 2014;7(1):26–30
- Oshika T, Nagahara K, Yaguchi S, Emi K, Takenaka H,
Tsuboi S, et al . Three year prospective
randomized evaluation of intraocular lens implantation through 3.2 and 5.5
mm incisions. J Cataract Refract Surg 1998;24:509-14
- Gokhale NS, Sawhney S. Reduction in astigmatism in
manual MSICS through change in astigmatism site. Indian J Ophthalmol
2005;53:201-3
- George R, Rapauliha P, Sripriya AV, Rajesh PS, Vahan PV,
Praveen S. Comparision of endothelial cell loss and surgically induced
astigmatism following conventional extracapsular cataract surgery, manual
small incision surgery and phacoemulsification. Ophthal Epidemiol
2005;12:293-7.
- Gogate PM, Kulkarni SR, Krishnaiah S, Deshpande RD,
Joshi SA, Palimkar A, et
al . Safety and efficacy
of phacoemulsification compared with manual small incision cataract
surgery by a randomized controlled clinical trial: Six weeks results.
Ophthalmology 2005;112:869-7411.
- Gogate P, Deshpande
M, Nirmalan PK. Why do phacoemulsification? Manual small-incision cataract
surgery is almost as effective, but less expensive. Ophthalmology
2007;114:965–8.
- Gogate PM,
Kulkarni SR, Krishnaiah S, et al. Safety and efficacy of
phacoemulsification compared with manual small-incision cataractsurgery by
a randomized controlled clinical trial: six-week results. Ophthalmology
2005;112:869–74.
- Ruit S, Tabin G,
Chang D, et al. A prospective randomized clinical trial of
phacoemulsification vs manual sutureless small-incision extracapsular
cataract surgery in Nepal. Am J Ophthalmol 2007;143:32–8.
It's a nice article, which you have shared here about phacoemulsification. Your article is very useful for those who are looking for a phacoemulsification course. I would like to thanks you for sharing this post here. phacoemulsification training in india
ReplyDelete